Learn about our Improving the Odds for Adolescents project.
Vulnerable Teens
Adolescence is a critical period for mental, social, and emotional wellbeing and development. During adolescence, the brain undergoes significant developmental changes, establishing neural pathways and behavior patterns that will last into adulthood. 1
Because their brains are still developing, adolescents are particularly receptive to the positive influences of youth development strategies, social and emotional learning, and behavioral modeling. But adolescents’ developing brains, coupled with hormonal changes, make them more prone to depression and more likely to engage in risky and thrill-seeking behaviors than either younger children or adults. These and other factors underline the importance of meeting the mental, social, and emotional health needs of this age group.
Mental health and social and emotional wellbeing – combined with sexual and reproductive health, violence and unintentional injury, substance use, and nutrition and obesity – form part of a complex web of potential challenges to adolescents’ healthy emotional and physical development.
Facts about Adolescent Mental Health
- Approximately 20% of adolescents have a diagnosable mental health disorder.
- Many mental health disorders first present during adolescence.
- — Between 20% and 30% of adolescents have one major depressive episode before they reach adulthood.— For a quarter of individuals with mood disorders like depression, these first emerge during adolescence.— Between 50% and 75% of adolescents with anxiety disorders and impulse control disorders (such as conduct disorder or attention-deficit/hyperactivity disorder) develop these during adolescence.
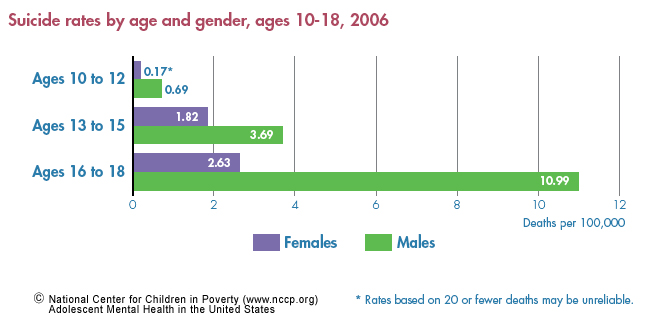
Figure 1: Suicide rates by age and gender, ages 10-18, 2006 - Suicide is the third leading cause of death in adolescents and young adults.
- — Suicide affects young people from all ages, races, genders, and socioeconomic groups, although some groups seem to have higher rates than others.— Older adolescents (aged 15-19) are at an increased risk for suicide (7.31/100,000).— Between 500,000 and one million young people aged 15 to 24 attempt suicide each year.
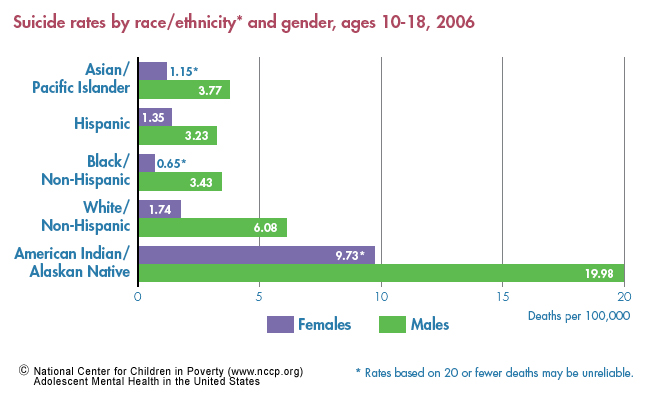
Figure 2: Suicide rates by race/ethnicity and gender, ages 10-18, 2006 - Existing mental health problems become increasingly complex and intense as children transition into adolescence.
- Untreated mental health problems among adolescents often result in negative outcomes.
- — Mental health problems may lead to poor school performance, school dropout, strained family relationships, involvement with the child welfare or juvenile justice systems, substance abuse, and engaging in risky sexual behaviors.— An estimated 67% to 70% of youth in the juvenile justice system have a diagnosable mental health disorder.
System-level Challenges to Attaining Adolescent Mental Health
Between 25% and 33% of adolescents forgo needed care, and many others lack access. Below are some of the factors hindering adolescents’ uptake of or access to programs and services that can help reduce the risk of mental health problems:
- Lack of access and utilization:
- — Health and health-related services access and use among adolescents lag behind that of other children.— Among adolescents with mental health needs, 70% do not receive needed care.
- Lack of adequate insurance coverage:
- — Adolescents represented more than 25% of the estimated 8.3 million uninsured children in 2005.— Nearly half of State Child Health Insurance Program (SCHIP) programs place limits on inpatient and outpatient mental health services.
- Lack of referral services and specialists trained in dealing with adolescents’ specialized needs:
- — Of the 213 accredited pediatric residency training 25 have fellowship programs in adolescent medicine, 7 of which include interdisciplinary training.
- Lack of stable living conditions:
- — Rates of serious mental health disorders among homeless youth range from 19% to 50%.— Homeless youth have a high need for treatment but rarely use formal treatment programs for medical, mental, and substance use services.
- Lack of confidentiality:
- — Laws in only 20 states and the District of Columbia give minors explicit authority to consent to outpatient mental health services.— There is a high prevalence of depressive symptoms, suicidal thoughts, and suicide attempts among adolescents who forgo care due to confidentiality concerns.
Recommendations
A well-financed health prevention and response system that fosters communication and cooperation across sectors can provide adolescents better access to high quality resources that are responsive to their unique mental health needs. In order to achieve this, federal and state governments should:
- Fund programs for adolescents that foster improved decision-making skills and provide positive models for behavior to reduce risk-taking behaviors. Adolescents are particularly resourceful and resilient and respond well to positive engagement strategies that help provide a social support structure.
- Provide funding to replicate comprehensive school-based health centers throughout the state, particularly those that provide mental health services. Access to on-site, school-based mental health services in school-based health centers increases the likelihood that adolescents will receive mental health services.
- Finance effective, empirically based prevention and early intervention strategies for health and behavioral health in schools. At least $700 billion is spent annually in the United States on preventable adolescent health problems.
- Finance effective, empirically based education programs to help parents recognize mental health problems in their children. When parents lack knowledge of teens’ mental health problems, obtaining services may be difficult.
- Pass legislation to enhance confidentiality protection to improve adolescents’ access to confidential services. Inconsistent and unclear policies regarding adolescent patient confidentiality can create additional barriers to mental health care. Only 45% of adolescents surveyed would seek care for depression if parental notification were required.
- Provide funding to attract, train, and retain a more diverse workforce of health care providers. Cultural differences between patient and provider can lead to misdiagnosis of major mental illness, while ethnic and gender matching has been shown to lead to lower dropout rates in mental health treatments.
- Establish local, state, and national targets for expanding the number of adolescent specialists in primary health, mental health, behavioral health, and addiction strategies. Data show that less than 1% of primary care physicians who may see adolescents are board-certified specialists in adolescent medicine.
- Institute financing mechanisms to support necessary services, especially in venues that increase access, such as schools, youth centers, and adolescent specific health and wellness centers. Insurance restrictions, poor funding, and low priorities for resources are among the key obstacles impeding access of children and adolescents to the services necessary to treat mental health disorders.
This fact sheet is supported by a generous grant from The Atlantic Philanthropies.
Endnotes
The author thanks Lola Adedokun, Ayana Douglas-Hall, and Rachel Masi for their contributions in writing this fact sheet.
1. National Research Council and Institute of Medicine. 2007. Challenges in Adolescent Health Care: Workshop Report. Committee on Adolescent Health Care Services and Models of Care for Treatment, Prevention, and Healthy Development. Board on Children, Youth, and Families, Division of Behavioral and Social Sciences and Education. Washington, DC: The National Academies Press. p. 1.
2. National Research Council and Institute of Medicine. 2002. Community Programs to Promote Youth Development. Committee on Community-Level Programs for Youth. Board on Children, Youth, and Families, Division of Behavioral and Social Sciences and Education. J. Eccles; J. A. Gootman (eds.). Washington, DC: National Academy Press.
3. Steinberg, L.; Dahl, R.; Keating, D.; Kupfer, D. J.; Masten, A. S.; Pine, D. 2004. The Study of Developmental Psychopathology in Adolescence: Integrating Affective Neuroscience with the Study of Context (Draft manuscript, Aug. 2003). Handbook of Developmental Psychopathology. D. Cicchetti, (ed.). John Wiley & Sons, New York. www.nyas.org/ebriefreps/ebrief/000219/archives/Developmental-Handbook.pdf (accessed March 31, 2009).
4. Beatty, A.; Chalk, R. 2007. A Study of Interactions: Emerging Issues in the Science of Adolescence. Program Committee for a Workshop on the Synthesis of Research on Adolescent Health and Development, Board on Children, Youth, and Families, Division of Behavioral and Social Sciences and Education. National Research Council and Institute of Medicine. Washington, DC: The National Academies Press. p. 8.
5. Kessler, R. C.; Berglund, P.; Demler, O.; Jin, R.; Walters, E. E. 2005. Life-time Prevalence and Age-of-onset Distribution of DSM-IV Disorders in the National Co-morbidity Survey Replication. Archives of General Psychiatry 62: 593-602.
7. Rushton, J. L.; Forcier, M.; Schectman, R. M. 2002. Epidemiology of Depressive Symptoms in the NationalLongitudinal Study of Adolescent Health. Journal of the American Academy of Child and Adolescent Psychiatry 4: 199-205.
10. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System (WISQARS). www.cdc. gov/ncipc/wisqars (accessed Sept. 2007).
11. National Adolescent Health Information Center. 2006. Fact Sheet on Suicide: Adolescents & Young Adults. San Francisco, CA: University of California, San Francisco. www.nahic.ucsf.edu/downloads/Suicide.pdf (accessed March 31, 2009).
13. Children’s Mental Health Statistics, Mental Health America. Mental Health America website. www1.nmha.org/children/prevent/stats.cfm (accessed March 31, 2009).
14. Patel, V.; Flisher, A. J.; Hetrick, S.; McGorry, P. 2007. Mental Health of Young People: A Global Public-health Challenge. Lancet 369(9569): 1302-13.
15. Kapphahn, C.; Morreale, M.; Rickert, V.; Walker, L. 2006. Financing Mental Health Services for Adolescents: A Position Paper of the Society for Adolescent Medicine. Journal of Adolescent Health 39: 456-458.
16. Skowyra, K. R.; Cocozza, J. J. 2006. Blueprint for Change: A Comprehensive Model for the Identification and Treatment of Youth with Mental Health Needs in Contact with the Juvenile Justice System . Delmar, NY: The National Center for Mental Health and Juvenile Justice and Policy Research Associates, Inc.
17. Klein, J. D. 1997. The National Longitudinal Study on Adolescent Health. Preliminary Results: Great Expectations. Journal of the American Medical Association 278(10), 864-965.
18. Fuentes-Affleck, E. 2006. Is Limited Access to Care the New Morbidity for Latino Young Adults? Journal of Adolescent Health (39)5: 623-624.
19. Yu, S. M.; Bellamy, H. A.; Kogan, M. D.; Dunbar, .J. L; Schwalberg, R.H., Schuster, M. A. 2002. Factors that influence receipt of recommended preventive pediatric health and dental care. Pediatrics, 110(6): e73.
20. Chandra, A.; Minkovitz, C. S. 2006. Stigma Starts Early: Gender Differences in Teen Willingness to Use Mental Health Services. Journal of Adolescent Health 38: 754e.1-754e8.
21. Center for Financing, Access and Cost Trends. 2005. Total Population and Uninsured Persons Under Age 65: Percent by Selected Population Characteristics, United States, First Half of 2005 (Table 1). (accessed Dec. 11, 2006).
22. Rosenbach, M.; Ellwood, M.; Irvin, C.; Young, C.; Conroy, W.; Quinn, B.; Kell, M. 2003. Implementation of the State Children’s Health Insurance Program: Synthesis of State Evaluations, Background for the Report to Congress. Washington, DC: Mathematica Policy Research, Inc., for Centers for Medicare and Medicaid Services, Department of Health and Human Services.
23. National Research Council and Institute of Medicine. 2007. Challenges in Adolescent Health Care Workshop Report, Committee on Adolescent Health Care Services and Models of Care for Treatment, Prevention, and Healthy Development. Board on Children, Youth, and Families, Division of Behavioral and Social Sciences and Education. Washington, DC: The National Academies Press, p. 21.
24. Robertson, M. J.; Toro, P. A. 1999. Homeless Youth: Research, Intervention, and Policy, from Practical Lessons: The 1998 National Symposium on Homelessness Research, L.B. Fosburg; D. B. Dennis (eds.). Washington, DC: U.S. Department of Housing and Urban Development, p. 3-1−3-32.
25. Farrow, J. A.; Deisher, M. D.; Brown, M. D.; Kulig, M. D.; Kipke, M. D. 1992. Health and Health Needs of Homeless and Runaway Youth. Journal of Adolescent Health 13: 717-726.
26. Kennedy, M. R. 1991. Homeless and Runaway Youth Mental Health Issues: No Access to the System. Journal of Adolescent Health 12: 576-579.
27. Boonstra, H.; Nash, E. 2000. Minors and the Right to Consent to Health Care, The Guttmacher Institute. www.guttmacher.org/pubs/tgr/03/4/gr030404.pdf (accessed April 6, 2009).
28. Lehrer, J.A.; Pantell, R.; Tebb, K.; Shafer, M.A. 2007. Forgone Health Care Among U.S. Adolescents: Associations Between Risk Characteristics and Confidentiality concern. Journal of Adolescent Health 40(3): 218-226.
29. Masten, A. S. 2007. Competence, Resilience, and Development in Adolescence: Clues for Prevention Science, from Adolescent Psychopathology and the Developing Brain: Integrating Brain and Prevention Science. D. Romer; E. F. Walker (eds.), New York: Oxford University Press.
30. Juszczak, L.; Melinkovich, P.; Kaplan, D. 2003. Use of Health and Mental Health Services by Adolescents Across Multiple Delivery Sites. Journal of Adolescent Health 32S: 108-118.
31. Kaplan, D.W.; Calonge, B.N.; Guernsey, B.P.; Hanrahan, M.B. 1998. Managed Care and SBHCs: Use of Health Services. Archives of Pediatrics and Adolescent Medicine 152(1): 25-33.
32. Hedberg, V.A.; Bracken, A.C.; Stashwick, C.A. 1999. Long-term Consequences of Adolescent Health Behaviors: Implications for Adolescent Health Services. Adolescent Medicine: State of the Art Reviews 10(1): 137-151.
33. Wu, P.; Hoven, C. W.; Bird, H. R.; Moore, R. E.; Cohen, P.; Alegria, M.; Dulcan, M. K.; Goodman, S. H.; Horwitz, S. M.; Lichtman, J. H.; Narrow, W. E.; Rae, D. S.; Regier, D. A.; Roper, M. T. 1999. Depressive and Disruptive Disorders and Mental Health Service Utilization in Children and Adolescents. Journal of the American Academy of Child and Adolescent Psychiatry 38(9): 1081-1090.
34. Ford, C.; English, A.; Sigman, G. 2004. Confidential Health Care for Adolescents: Position Paper of the Society for Adolescent Medicine. Journal of Adolescent Health 35: 160-167.
35. Issues at a Glance: Adolescent Access to Confidential Health Services, Advocates for Youth. Advocates for Youth website. (accessed March 31, 2009.
36. Jones, B. E.; Gray, B. A. 1986. Problems in Diagnosing Schizophrenia and Affective Disorders among Blacks. Hospital and Community Psychiatry 37: 61-65.
37. Sue, S.; Fujino, D. C.; Hu, L.; Takeuchi, D. T.; Zane, N. W. S. 1991. Community Mental Health Services for Ethnic Minority Groups: A Test of the Cultural Responsiveness Hypothesis. Journal of Consulting and Clinical Psychology 59: 533–540.
38. National Research Council and Institute of Medicine. 2007. Challenges in Adolescent Health Care: Workshop Report. Committee on Adolescent Health Care Services and Models of Care for Treatment, Prevention, and Healthy Development. Board on Children, Youth, and Families, Division of Behavioral and Social Sciences and Education. Washington,DC: The National Academies Press. p. 7.
39. Mental Health: A Report of the Surgeon General. 1999. Rockville, MD: Department of Health and Human Services.
40. Kapphahn, C.; Morreale, M.; Rickert, V.; Walker. L. 2006. Financing Mental Health Services for Adolescents: A Position Paper of the Society for Adolescent Medicine. Journal of Adolescent Health 39: 456-458.
41. Kapphahn, C.; Morreale, M.; Rickert, V.; Walker. L. 1998. Meeting the Health Care Needs of Adolescents in Managed Care: A Position Paper of the Society for Adolescent Medicine. Journal of Adolescent Health 22: 271-277.