Learn about our Improving the Odds for Adolescents project.
The reproductive and sexual health needs of adolescents differ from those of adults. During adolescence, the body undergoes significant developmental changes, most notably puberty, the bodily changes of sexual maturation, and the formation of sexual identity. Achieving reproductive and sexual health requires more than preventing unwanted pregnancy and sexually transmitted infections, it includes developing the ability to form and maintain meaningful relationships with others and with one’s own body. Psychological, social, educational, environmental, and economic factors, among others, all play a role. In addition, adolescents are more likely to engage in risk-taking behaviors than either younger children or adults. These significant factors underline the importance of meeting the reproductive and sexual health needs of this age group.
Reproductive and sexual health – combined with mental health disorders and emotional problems, violence and unintentional injury, substance use, and poor nutrition – form part of a complex web of potential challenges to adolescents’ healthy emotional and physical development.
Facts About Sexual and Reproductive Health
United States teen pregnancy, birth, abortion, and sexually transmitted disease rates are higher than those in most other developed countries, and rising. Factors associated with teen fertility and risky sexual behavior include socioeconomic status, parental education, community and peer influences, self-esteem, access to education, and school success, among many others.
Pregnancy
- After a 14-year decline, birth rates for teens age 15 to 19 increased three percent in 2006 (to 41.9 per 1,000), though rates vary by race.
- Teen mothers are more likely to drop out of school and face unemployment, poverty, welfare dependency, and other negative outcomes than women who delay childbearing.
Sexual Activity
- After a decade of decline, rates of sexual activity among high school students have been rising since 2001 and vary by gender and race.
- – Among male high school students, 73 percent of blacks, 58 percent of Hispanics, and 44 percent of whites reported having had sexual intercourse in 2007.– Among female high school students, 61 percent of blacks, 46 percent of Hispanics, and 43.7 percent of whites reported having had sexual intercourse in 2007.
- After over a decade of growth, rates of condom usage among high school students have been declining since 2003 and vary by gender and race.
- – Among male high school students, 74 percent of blacks, 70 percent of Hispanics, and 66.4 percent of whites reported using a condom at last intercourse in 2007.– Among female high school students, 60 percent of blacks, 52 percent of Hispanics, and 53.9 percent of whites reported their partner using a condom at last intercourse in 2007.
Relationships
- About one in five high school girls has been physically or sexually abused by a dating partner.
- – Dating abuse is associated with unhealthy sexual behaviors that can lead to unintended pregnancy, sexually transmitted diseases, and HIV infections.– Dating abuse occurs more frequently among black students (13.9 percent) than among Hispanic (9.3 percent) or white (7.0 percent) students.
- About 10 percent of adolescent females experience non-voluntary first sex.
Sexually Transmitted Diseases
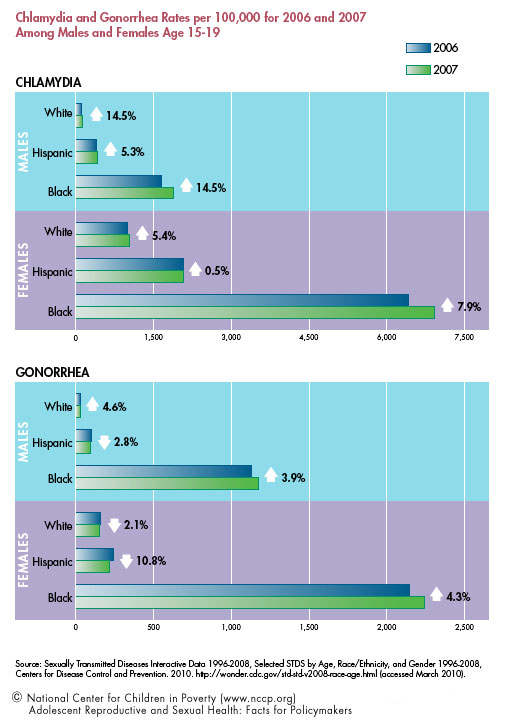
- In 2007, chlamydia and gonorrhea rates increased for both females and males age 15 to 19, but varied by gender and race.
- – Females in this age group had the highest rates of chlamydia and gonorrhea compared to any other age or sex group and showed 6.4 percent and 1.4 percent increases respectively from the previous year.– Males had lower rates of chlamydia and gonorrhea than females but showed 14.3 percent and 3.8 percent increases respectively from the previous year.
- About 35 percent of 14 to 19 year olds test positive for high-risk human papillomavirus, a virus linked to cervical cancer in women.
- In 2007, adolescents represented four percent of all new cases of HIV infections in the U.S.
System-level Challenges to Attaining Adolescent Sexual and Reproductive Health
Between 25 and 33 percent of adolescents forgo needed care and many others lack access. Below are some of the factors hindering adolescents’ use of or access to programs and services that can help reduce the risk of sexual and reproductive health problems:
- Lack of confidentiality.
- – Inconsistent and unclear policies regarding adolescent patient confidentiality can create additional barriers to care.– While 60 percent of adolescents seeking reproductive health services at family planning clinics do so with parental knowledge, one in five would use no contraception or the withdrawal method only if parental notification for prescription contraceptives were mandated.– Adolescents who take health risks and experience psychological distress are more likely to forgo health care due to confidentiality concerns despite being among the most vulnerable and in need of health care services.
- Lack of access and utilization to preventive care.
- – Among all children and youth, adolescents were the least likely to attend preventive well-child visits based on medical recommendations.– Adolescents’ low rates of outpatient visits put them at increased risk for health complications, and high school dropouts are at even greater risk than their non-dropout peers.
- Lack of adequate insurance coverage.
- – Adolescents and young adults are more likely to be uninsured than any other age group, with 16.2 percent between the ages of 13 and 17 lacking any insurance.
- Lack of providers trained in adolescent health.
- – Of the 195 accredited pediatric residency training programs in the U.S., only 27 have fellowship programs to train clinicians in adolescent care.
- Lack of comprehensive sexuality education.
- – Fewer than half of all states require public schools to teach sex education and fewer than one-third require the curriculum to cover contraception.
Recommendations
The newly charged federal Office of Adolescent Health should take the lead in fostering cross-sector collaboration and supporting comprehensive health programs, providing all adolescents better access to high quality services that are responsive to their unique needs. Specifically, both federal and state governments should:
- Fund positive youth development and afterschool programs. Positive youth development programs have been found to reduce sexual risk behaviors in adolescents. High quality afterschool programming improves academic achievement and youths’ attitudes towards school, factors associated with delayed onset of sexual activity.
- Fund programs that bring services to youth who are disconnected from school, employment, and social supports. Research suggests that integrating health promotion and disease prevention into youth employment and training programs can improve health and employment outcomes for disconnected youth, a group with particularly poor health status and low insurance coverage.
- Support programs that educate and empower young people as peer educators and advocates. Research shows that peer leaders can be more effective than adults in establishing conservative norms and attitudes related to sexual behavior.
- Provide funding to establish and expand school-based health centers, particularly those that provide comprehensive primary care services. Access to on-site, school-based health centers increases the likelihood that adolescents will receive health and counseling services.
- Pass legislation to enhance confidentiality protection to improve adolescents’ access to confidential services. Inconsistent and unclear policies regarding adolescent patient confidentiality can create additional barriers to care.
- Finance mechanisms to allow foster youth to voluntarily retain state guardianship with appropriate services and supports up to age 25. Former foster youth more frequently experience episodes of homelessness and survival sex.
- Make contraceptives widely available in venues frequented by adolescents, including schools. Sexually active adolescents in schools where condoms were available were more likely to report having used condoms in their most recent sexual encounter.
This fact sheet is supported by a generous grant from The Atlantic Philanthropies.
Endnotes
1. Promoting the Sexual and Reproductive Health of Adolescents, World Health Organization, 2010. World Health Organization website. www.who.int/reproductivehealth/topics/adolescence/en/index.html (accessed March 2010).
2. Puberty, National Institute of Child Health and Human Development, National Institutes of Health. 2007. National Institutes of Health website. www.nichd.nih.gov/health/topics/puberty.cfm (accessed March 2010).
3. Tolman, Deborah L.; Striepe, Meg I.; Harmon, Tricia. 2003. Gender Matters: Constructing a Model of Adolescent Sexual Health. The Journal of Sex Research 40(1): 4-12. www.jstor.org/stable/3813766 (accessed March 2010).
4. Steinberg, Laurence; Dahl, Ronald; Keating, Daniel; Kupfer, David J.; Masten, Ann S.; Pine, Daniel S. 2004. The Study of Developmental Psychopathology in Adolescence: Integrating Affective Neuroscience with the Study of Context (Draft manuscript, Aug. 2003). Handbook of Developmental Psychopathology.D. Cicchetti, (ed.). John Wiley & Sons, New York. www.nyas.org/ebriefreps/ebrief/000219/archives/DevelopmentalHandbook.pdf(accessed March 2009).
5. Beatty, A.; Chalk, R. 2007. A Study of Interactions: Emerging Issues in the Science of Adolescence. Program Committee for a Workshop on the Synthesis of Research on Adolescent Health and Development, Board on Children, Youth, and Families, Division of Behavioral and Social Sciences and Education. National Research Council and Institute of Medicine. Washington, DC: The National Academies Press. p. 8.
6. Singh, S.; Darroch, J. E. 2000. Adolescent Pregnancy and Childbearing: Levels and Trends in Developed Countries. Family Planning Perspectives32(1):14–23.
Santelli, John S.; Melnikas, Andrea J. 2010. Teen Fertility in Transition: Recent and Historic Trends in the United States. Annual Review of Public Health 31.
Ethier, Kathleen A.; Kershaw, Trace S.; Lewis, Jessica B.; Milan, Stephanie; Niccolai, Linda M.; Ickovics, Jeannette R. 2006. Self-esteem, Emotional Distress and Sexual Behavior Among Adolescent Females: Inter-relationships and Temporal Effects. Journal of Adolescent Health 38(3): 268-274.
8. Martin, Joyce A.; Hamilton, Brady E.; Sutton, Paul D.; Ventura, Stephanie J.; Menacker, Fay; Kirmeyer, Sharon; Mathews, T. J. 2009. Centers for Disease Control and Prevention. Births: Final Data for 2006. National Vital Statistics Reports 57(7).
9. Hoffman, Saul D. 2006. By the Numbers: The Public Costs of Teen Childbearing. Washington, DC: National Campaign to Prevent Teen Pregnancy.
10. United States 2007 Percentage of Students Who Ever Had Sexual Intercourse, Youth Risk Behavior Survey, Centers for Disease Control and Prevention. 2008. Centers for Disease Control and Prevention website. http://apps.nccd.cdc.gov/yrbss/ (accessed March 2010).
13. United States 2007 Among Students Who Were Currently Sexually Active, The Percentage Who Reported That Either They or Their Partner Had Used a Condom During Last Sexual Intercourse, Youth Risk Behavior Survey, Centers for Disease Control and Prevention. 2008. Centers for Disease Control and Prevention website. http://apps.nccd.cdc.gov/yrbss/ (accessed March 2010).
16. Silverman, Jay G.; Raj, Anita; Mucci, Lorelei A.; Hathaway, Jeanne E. 2001. Dating Violence Against Adolescent Girls and Associated Substance Use, Unhealthy Weight Control, Sexual Risk Behavior, Pregnancy, and Suicidality. Journal of the American Medical Association 286(5):572–9.
18. Centers for Disease Control and Prevention. 2006. Physical Dating Violence Among High School Students – United States, 2003. Morbidity and Mortality Weekly Report 55(19): 532-535.
19. Abma, Joyce C.; Martinez, Gladys M.; Mosher, William D.; Dawson, Brittany S. 2004. Teenagers in the United States: Sexual Activity, Contraceptive Use, and Childbearing, 2002. National Center for Health Statistics. Vital and Health Statistics 23(24).
20. STDs in Adolescents and Young Adults, Sexually Transmitted Diseases Surveillance, 2007, Centers for Disease Control and Prevention. 2009. Centers for Disease Control and Prevention website. www.cdc.gov/std/stats07/adol.htm (accessed March 2010).
22. Sexually Transmitted Diseases Interactive Data 1996-2008, Selected STDS by Age, Race/Ethnicity, and Gender 1996-2008, Centers for Disease Control and Prevention. 2010. http://wonder.cdc.gov/stdstd-v2008-race-age.html(accessed March 2010).
23. Other Sexually Transmitted Diseases, Sexually Transmitted Diseases Surveillance, 2007. Centers for Disease Control and Prevention. 2009. Centers for Disease Control and Prevention website. www.cdc.gov/STD/stats07/other.htm (accessed March 2010).
24. Basic Statistics, Centers for Disease Control and Prevention. 2009. Centers for Disease Control and Prevention website. www.cdc.gov/hiv/topics/surveillance/basic.htm#hivaidsage (accessed Oct. 2009).
25. Klein, Jonathan D. 1997. The National Longitudinal Study on Adolescent Health. Preliminary Results: Great Expectations. Journal of the American Medical Association 278(10), 864-865.
26. Fuentes-Affleck, E. 2006. Is Limited Access to Care the New Morbidity for Latino Young Adults? Journal of Adolescent Health (39)5:623-624.
27. Ford, Carol; English, Abigail; Sigman, Garry. 2004. Confidential Health Care for Adolescents: Position Paper of the Society for Adolescent Medicine. Journal of Adolescent Health 35(2): 160-167.
28. Jones, Rachel K.; Purcell, Alison; Singh, Susheela.; Finer, Lawrence B. 2005. Adolescents’ Reports of Parental Knowledge of Adolescents’ Use of Sexual Health Services and Their Reactions to Mandated Parental Notification for Prescription Contraception. Journal of the American Medical Association293(3): 340-8.
29. Lehrer, Jocelyn, A.; Pantell, Robert; Tebb, Kathleen; Shafer, Mary-Ann. 2007. Forgone Health Care Among U.S. Adolescents: Associations between Risk Characteristics and Confidentiality Concern. Journal of Adolescent Health 40(3): 218-226.
30. Selden, Thomas M. 2006. Compliance with Well-child Visit Recommendations: Evidence from the Medical Expenditure Panel Survey, 2000-2002. Pediatrics 118(6): e1766-e1778.
31. Ma, Jun; Wang, Yun; Stafford, Randall S. 2005. US Adolescents Receive Suboptimal Preventive Counseling During Ambulatory Care. Journal of Adolescent Health 36(5): 441e1-441e7.
Tandon, S. Darius; Marshall, Beth; Templeman, Amy J.; Sonenstein, Freya L. 2008. Health Access and Status of Adolescents and Young Adults Using Youth Employment and Training Programs in an Urban Environment. Journal of Adolescent Health 43(1): 30-37.
32. Total Population and Uninsured Persons Under Age 65: Percent by Selected Population Characteristics, United States, First Half of 2007, MedicalExpenditure Panel Survey, Agency for Healthcare Research and Quality. 2007. Medical Expenditure Panel Survey Home website. www.meps.ahrq.gov/mepsweb/ (accessed Oct. 2009).
33. Number of Accredited Programs for the Current Academic Year (2009-2010), Accreditation Council for Graduate Medical Education. Accreditation Council for Graduate Medical Education website. www.acgme.org/adspublic/(accessed July 2009).
Training Opportunities in Adolescent Medicine – 2010, The Society for Adolescent Medicine. The Society for Adolescent Medicine website. www.adolescenthealth.org/TrainingOpportunities-AdolescentMedicine.pdf(accessed July 2009).
34. State Policies in Brief: Sex and STI/HIV Education, Guttmacher Institute. 2010. Guttmacher Institute website. www.guttmacher.org/statecenter/spibs/spib_SE.pdf (accessed March 2010).
35. Gavin, Loretta E.; Catalano, Richard F.; David-Ferdon, Corinne; Gloppen, Kari M.; Markham, Christine M. 2010. A Review of Positive Youth Development Programs That Promote Adolescent Sexual and Reproductive Health. Journal of Adolescent Health 46(3): S75-S91.
36. Masten, Ann S. 2007. Competence, Resilience, and Development in Adolescence: Clues for Prevention Science, from Adolescent Psychopathology and the Developing Brain: Integrating Brain and Prevention Science. Daniel Romer; Elaine Walker (eds.). New York: Oxford University Press.
Durlak, J.; Weissberg, R. 2007. The Impact of Afterschool Programs That Promote Personal and Social Skills. Chicago, IL: Collaborative for Academic, Social, and Emotional Learning.
37. Tandon, S. Darius; Marshall, Beth; Templeman, Amy J.; Sonenstein, Freya L. 2008. Health Access and Status of Adolescents and Young Adults Using Youth Employment and Training Programs in an Urban Environment. Journal of Adolescent Health 43(1): 30-37.
38. Mellanby, A. R.; Newcombe, R. G.; Rees, J.; Tripp, J. H. 2001. A Comparative Study of Peer-led and Adult-led School Sex Education. Health Education Research: Theory and Practice 16(4): 481-492.
Mellanby, A. R.; Rees, J.; Tripp, J. H. 2001. Peer-led and Adult-led School Health Education: A Critical Review of Available Comparative Research. Health Education Research: Theory and Practice 15(5):533-545.
39. Juszczak, Linda; Melinkovich, P.; Kaplan, D. 2003. Use of Health and Mental Health Services by Adolescents Across Multiple Delivery Sites. Journal of Adolescent Health 32S: 108-118.
40. Ford, Carol; English, Abigail; Sigman, Garry. 2004. Confidential Health Care for Adolescents: Position Paper of the Society for Adolescent Medicine. Journal of Adolescent Health 35(2): 160-167.
41. Courtney, Marc. 2005. Network on Transitions to Adulthood Policy Brief. MacArthur Foundation Research Network on Transitions to Adulthood and Public Policy. www.transad.pop.upenn.edu/downloads/courtney–foster%20care.pdf (accessed July 2009)
42. Blake, Susan M.; Ledsky, Rebecca; Goodenow, Carol; Sawyer, Richard; Lohrmann, David; Windsor, Richard. 2003. Condom Availability Programs in Massachusetts High Schools: Relationships with Condom Use and Sexual Behavior. American Journal of Public Health 93(6): 955-962.