Learn about our Improving the Odds for Adolescents project.
Adolescent obesity in the United States has many important implications for both the health and well-being of the individual and society. Specific negative impacts of obesity on health include increased susceptibility to a host of diseases, chronic health disorders, psychological disorders, and premature death, which in turn add billions of dollars in health care costs each year. Excess medical costs due to overweight adolescents are estimated at more than $14 billion per year. Furthermore, adolescent obesity affects our nation’s ability to protect itself; more than a quarter of 17- to 24-year-olds are not fit to enroll in the military due to their weight.
Adolescence is a crucial period for establishing healthy behaviors. Many of the habits formed during this developmental stage will last well into adulthood. Although obesity is a complex problem not yet fully understood by researchers, by addressing the known factors that contribute to obesity in adolescence, policymakers can help ensure a healthy and productive adulthood for our nation’s youth.
Obesity and poor nutrition – combined with mental health disorders and emotional problems, violence and unintentional injury, substance use, and reproductive health problems – form part of a complex web of potential challenges to adolescents’ healthy emotional and physical development.
Overweight and Obesity
Obesity and overweight are measured using Body Mass Index (BMI), a number calculated from a person’s weight and height that is a reliable indicator of body fatness for most children and adolescents. BMI for children and adolescents is gender- and age- specific because body fatness changes over the years as they grow and differs between males and females. Adolescents in the 85th to 94th percentile BMI are classified as overweight. Those in the 95th percentile or above are classified as obese.
Facts about Obesity and Nutrition
Prevalence
- One out of every six adolescents is overweight, and one out of every three is at risk.
- – Since the 1980s, the proportion of overweight children has steadily increased.
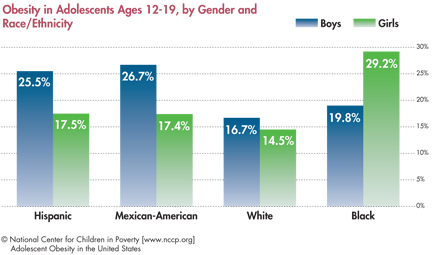
- Obesity rates vary by race/ ethnicity.
- – For adolescents ages 12 to 19, non-Hispanic black girls and Mexican-American boys have the highest rates of obesity, 29.2 percent and 26.7 percent respectively. Non-Hispanic white boys and girls have the lowest rates of obesity at 16.7 percent and 14.5 percent respectively.
- Childhood obesity was found to be highest in the Southeast, with eight of the 10 states with the highest rates of childhood obesity being in this region.
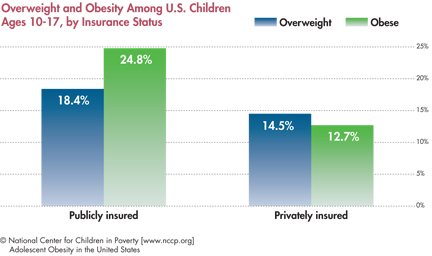
- In 2007, the prevalence of overweight and obesity was greater among publicly insured children ages 10 to 17 than their privately insured peers.
Lifestyle Factors
- Adolescents and their families eat more food prepared away from home than in the past.
- – When people eat outside the home, they consume more total calories per eating occasion than they do at home, and a higher proportion of those calories comes from saturated fats.
- According to USDA estimates, 116.3 million Americans, including adolescents, live in areas with low access to supermarkets.
- In 2009, less than 20 percent of high school students engaged in the recommended amount of physical activity of 60 minutes every day, and over 20 percent did not get 60 minutes of exercise on any day, though rates vary by gender and race.
Health Consequences
- Being overweight increases the risk of developing diabetes, heart disease, high blood pressure, and cancer, among other adverse outcomes.
- The current generation of children could potentially live shorter lives than their parents.
- Overweight adolescents are more likely to become overweight adults than their normal weight peers, with one study showing 80 percent of children who were overweight at 10 to 15 years were obese adults at age 25.
- Overweight and obese teenage mothers are at increased risk for gestational diabetes and caesarean delivery.
Economic Consequences
- The direct and indirect costs of the obesity epidemic exceed $140 billion annually.
- – The US spends six to 10 percent of healthcare spending on costs attributable to obesity, compared to two percent to 3.5 percent in other Western countries.– Data show obesity represents 27 percent of the rise in US healthcare costs over the past 20 years.
System-level Challenges to Preventing and Combating Adolescent Obesity
Below are some of the factors that contribute to increases in adolescent obesity, many of which are experienced to a greater degree by and have a greater impact on adolescents of color than their white peers.
- Limited access to healthy and affordable foods.
- Millions of Americans, many of whom are low-income or poor, live in areas lacking convenient access to fresh, healthy, and affordable foods.Limited access to healthy foods encourages poor food choices that have serious health consequences.
- Environment.
- – Close proximity of a fast food restaurant to schools is associated with increased obesity rates in adolescents.– Outside of government-regulated child nutrition programs, the foods sold to adolescents at schools are disproportionately high-fat snacks and sweetened beverages.
- Food insecurity.
- – In 2008, children, including adolescents, in more than 500,000 households ate less than they needed as a result of a lack of money.– Researchers believe that when a person is food insecure they choose inexpensive, unhealthy, calorie-dense foods and beverages.
- Poor eating habits.
- Adolescents consume more calories from sugar-sweetened beverages and fruit juices than in the past, and more than half of these beverages are consumed in the home.
- Food marketing targeting children and adolescents.
- Food marketers spent $1 billion in 2006 marketing food, much of it unhealthy, to adolescents using TV, Internet, and other media sources.
- Increases in “screen time.”
- – Even with bouts of physical activity, more time spent in front of a screen during adolescence is associated with increased obesity in both adolescence and young adulthood, and the association is greater among females than males.
- Decreased physical activity both inside and outside of school.
- – Between 1969 and 2001, the percentage of middle and high school students walking or biking to school decreased from 41.6 percent and 26.4 percent, respectively, to 15.2 percent and 8.1 percent.
Recommendations
Obesity is a complex, multifactor problem, and effective solutions require comparable sophistication. Although the causes of obesity have not been exhaustively and precisely characterized, there are choices policymakers can make to combat the problem and reduce its impact. As with most interventions, prevention typically trumps treatment, and policymakers should keep that in mind while developing policies. Closely guided by the comprehensive White House Task Force on Childhood Obesity Report to the President, we developed the following recommendations for local, state, and federal policymakers:
- Implement and enforce rules on nutritional information that make it easier for parents and adolescents to make healthy choices. Clear food and menu labeling can enable families to make better choices for themselves and their families.
- Increase access to healthy and affordable foods. A growing body of evidence suggests that increases in food store availability improve adolescent BMI. In addition, when the price of healthy foods is reduced, people consume more of them. Government can promote access through a variety of initiatives, such as providing tax credits for supermarkets and grocery stores in underserved communities and creating incentives to promote production of fruits and vegetables.
- Ensure that families who need food assistance have access to it. Policymakers can promote access to food assistance by simplifying the application process for food assistance programs, ensuring that people who qualify for these programs are aware of them, enabling the use of WIC and food stamps at greenmarkets, and providing subsidies for healthier foods.
- Limit childhood exposure to food marketing. Food advertising has been shown to strongly affect children’s food habits. By limiting advertisements for unhealthy foods targeting young people, policymakers can make it more likely that adolescents will make healthier decisions about food.
- Improve quality of and safeguard funding for school food programs. School represents a crucial opportunity for government to teach children and youth about and enable them to develop healthy eating habits. Improving the quality and reach of school food programs can tangibly improve the health of children.
- Improve quality of other foods sold at or near schools. Many foods are sold at school that are not subject to federal nutrition standards and typically contribute to poor nutritional choices.24 School food policies that decrease access to foods high in fats and sugars, such as restricting vending machine hours or limiting the types of food that are sold, are associated with less frequent purchase of high fat and sugar items among high school students.
- Increase opportunities for and access to physical activity, including support for evidence-based physical education curricula such as SPARK. Physical activity can reduce the risk of obesity and has numerous benefits that extend beyond just physical health, such as reducing depression symptoms and improving self-esteem.
- Partner with the private sector to encourage safe pedestrianand physical-activity-friendly development projects, especially in low-income communities.Making neighborhoods safer and more pedestrian-friendly can encourage physical activity and reduce the negative effects of our modern environment.
- Fund promising demonstration projects addressing disparities in obesity rates and further research into culturally responsive alternatives. Higher rates of obesity in ethnic minority groups compared to whites of the same socioeconomic status suggest that different strategies need to be developed to address obesity in different race and ethnic groups.