Learn about our Improving the Odds for Young Children project.
Young children’s health is essential to their overall development, well-being, and school readiness. Untreated health problems and a lack of preventive care contribute to higher rates of serious illness, absenteeism in preschool, physical and emotional distress, and even long-term disability. At a historic moment when the passage of federal health care reform promises significant improvements in health care access for many Americans, it is important to take stock of how well states are currently meeting the health needs of young children in low-income families. This brief presents information from NCCP’s Improving the Odds for Young Children project about state policy choices in the following areas that affect the health and well-being of children, ages birth to 5:
- access to health care and continuity of care;
- maternal health care; and
- preventive screening and assessment.
Relevant components of health care reform legislation are considered in a set of recommendations for meeting the short and long-term health care needs of young, low-income children.
Access to Health Care and Continuity of Care
Eligibility for Medicaid and the Child Health Insurance Program (CHIP)
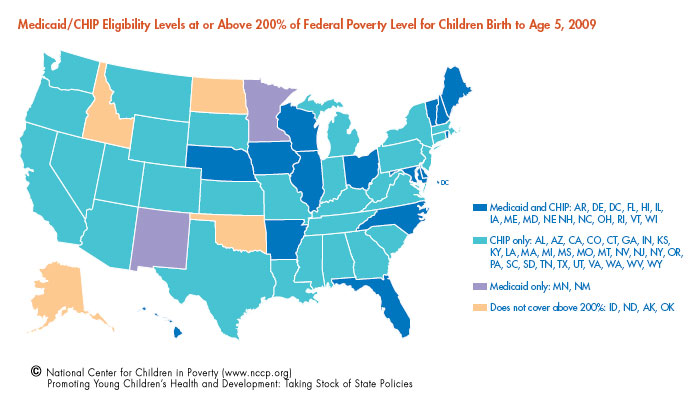
As a result of the CHIP expansion signed into law by President Obama in early 2009, children in households with income at or above 200 percent of the federal poverty line (FPL) have access to public health insurance (Medicaid/CHIP) in all but five states.
| 2009 Poverty Guidelines U.S. Department of Health and Human Services |
||
| Persons in Family or Household | ||
| 1 | 10,830 | |
| 2 | 14,570 | |
| 3 | 18,310 | |
| 4 | 22,050 | |
| 5 | 25,790 | |
| 6 | 29,530 | |
| 7 | 33,270 | |
| 8 | 37,010 | |
| For each additional person, add $3,740 | ||
- Currently, 46 states have set the income eligibility for Medicaid/CHIP at or above 200 percent of FPL for young children. In 2009, four states – Montana, Nebraska, Oregon and South Carolina – raised their eligibility thresholds to at least 200 percent of FPL. Ten states with previous levels already at 200 percent of FPL increased eligibility above 200 percent in 2009, ranging from 205 percent of FPL for children birth to age 5 in Colorado, to 400 percent of FPL for children birth to age 5 in New York. Arizona recently suspended its CHIP program that previously served children up to 200 percent of FPL.
- Alaska, Idaho, North Dakota, and Oklahoma have income eligibility ranging from 160 percent to 185 percent of FPL. Following the recent elimination of its CHIP program, Arizona now covers young children in families with incomes up to 140 percent of FPL (birth to age 1), and up to 133 percent of FPL (age 1 to 5) through Medicaid.
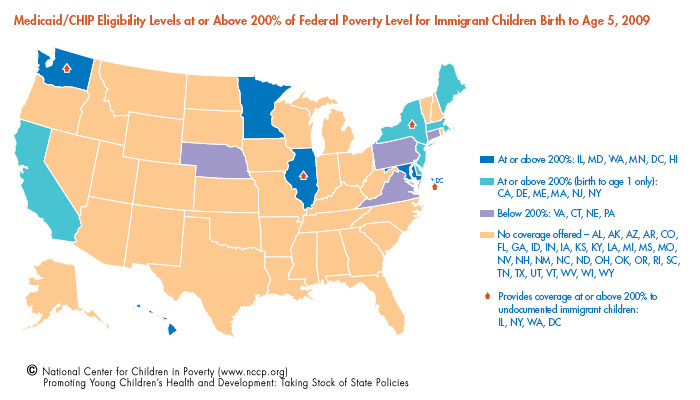
States can also provide public health insurance to immigrant children through a Medicaid option (for legal documented children only) and through separate state funds (for undocumented children). The relatively high rates of health problems among immigrant children age 5 and younger highlight their need for access to health care. In one study comparing the health status of poor immigrant and non-immigrant children, more than twice as many immigrant children were reported by parents to be in poor or fair health. While some states offer coverage to young immigrant children, this vulnerable group has much less access to health care than other low-income children.
- Twelve states offer coverage to all or most legal documented immigrant children birth to age 1 with household incomes at or above 200 percent FPL. Four of the 12 states – Illinois, New York, Washington, and the District of Columbia – also extend coverage to undocumented immigrant children birth to age 1.
- Six of the 12 states provide coverage to all or most legal immigrant children age 1 to 5 with household incomes at or above 200 percent FPL. Three of the six states – New York, Washington, and the District of Columbia – also extend coverage to most undocumented immigrant children age 1 to 5 with household incomes at or above 200 percent FPL.
Medical Homes for Young Children
Young children benefit from having a “medical home,” described by the American Academy of Pediatrics (AAP) as health care that is “accessible, continuous, comprehensive, family-centered, coordinated, compassionate, and culturally effective.” Research shows that public health insurance programs improve the physical health and development of children through the receipt of consistent and continuous health care. Children enrolled in public health insurance programs are also more likely to receive regular dental care and visit emergency rooms less often.
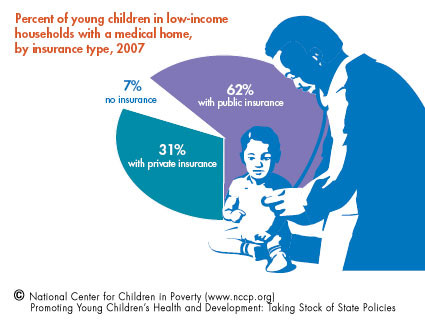
Medical home data released in 2009 suggest that young children in low-income households who have public insurance coverage are more likely to have a medical home. However, even among children covered by public insurance, too few have a medical home that can help ensure effective health care.
- Sixty-two percent of young children with public insurance have a medical home.
- Thirty-one percent of young children with private insurance have a medical home.
- Seven percent of young children with no insurance have a medical home.
States’ policies regarding continuity of public health care coverage may support or impede families’ ability to maintain a medical home for young children.
Continuity of Care
State policy choices affect the extent to which health care for young children and pregnant women is timely – available when most needed – and uninterrupted. In most states, the enrollment process for Medicaid and CHIP can be time consuming. The required, periodic re-enrollment process can result in eligible families losing coverage due to administrative lapses and paperwork errors.
- Forty-seven states require that children’s eligibility for Medicaid/CHIP be reviewed every 12 months. Thirty-one of these states have formal 12-month continuous eligibility policies, while six states employ policies similar to continuous eligibility but which do not meet all aspects of the formal policy.
- Four states – Georgia, Minnesota, Pennsylvania, and Texas – require review every six months for Medicaid.
- Only 14 states have policies known as “presumptive eligibility,” which provides temporary coverage for young children while their initial applications are being reviewed for approval. Nine of these states have implemented “presumptive eligibility” policies for both Medicaid and CHIP, while the remaining five states do so only for Medicaid.
- Three states – Alabama, Louisiana, and New Jersey – have established formal Express Lane Eligibility initiatives to automatically enroll children in Medicaid/CHIP when they qualify for other government programs. New York, Vermont, and Wisconsin have programs similar to Express Lane Eligibility but which do not meet all of the requirements.
Young Children’s Health and Well-being is Linked to Maternal Health
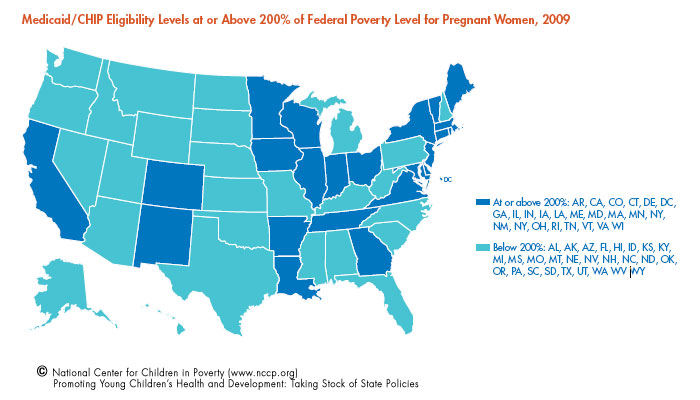
The health and well-being of infants and young children is closely tied to the health of pregnant women. It is especially important for pregnant women to receive prenatal care that includes screening for conditions such as periodontal disease, obesity and depression. These conditions are linked to increased risk for preterm births, low birth weight, preeclampsia, miscarriage, and poor physical and socio-emotional development of infants. Despite increased Medicaid/CHIP eligibility for low-income children, pregnant women in many states continue to lack access to public health insurance.
- Twenty-four states cover pregnant women at 200 percent of FPL or higher – an increase of four states.
- Ten states set the income eligibility at or below 150 percent of FPL for pregnant women.
- Seventeen states set the income eligibility between 175 percent and 185 percent of FPL for pregnant women.
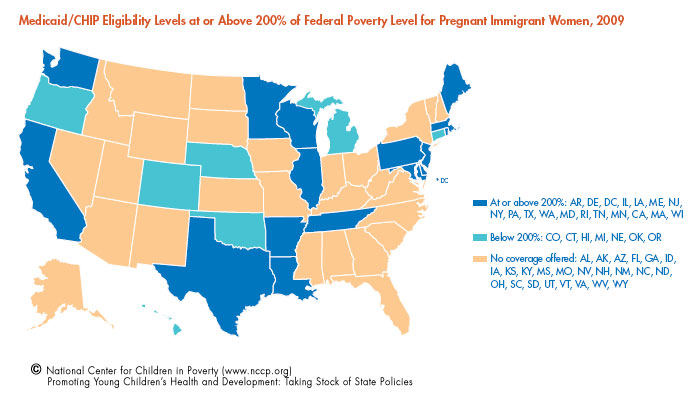
- Currently, 25 states offer public health insurance to pregnant immigrant women: 17 of these states offer coverage to all legal and undocumented immigrants, while eight states offer coverage to all or most legal immigrants.
- Eighteen states cover pregnant immigrant women with incomes at or above 200 percent of FPL.
Despite low eligibility levels in many states, pregnant women can be enrolled immediately in Medicaid through “presumptive eligibility” policies in 30 states. An additional five states have policies that are very similar to presumptive eligibility, allowing pregnant women to receive prenatal health care and screening before their applications are formally approved.
Well-child Visits and Preventive Screening

Even when young, low-income children have health insurance, they do not always receive the health, developmental and dental screenings that are consistent with pediatric practice recommendations, and key to preventing or reducing the severity of future problems. The Early and Periodic Screening, Diagnosis and Treatment (EPSDT) program is Medicaid’s comprehensive child health benefits package. EPSDT requires health care providers to periodically screen children for good health, diagnose any medical problems or delays, and provide treatment for identified conditions.
AAP recommends that children receive a set number of well-child medical visits per year: seven visits in the baby’s first year, four visits between the ages of 1 and 2 years, and three visits between the ages of 3 and 5 years. During these visits, parents receive important guidance about how to support their child’s health and development. EPSDT screens are also conducted in well-child visits. Many states are falling short of these guidelines, requiring fewer than the number of recommended visits.
- Only five states – Georgia, Indiana, North Dakota, Vermont, and West Virginia – met or exceeded AAP recommendations for seven well-child visits for a child birth to age 1.
- Thirty-nine states met AAP recommendations for four well-child visits for a child between the ages of 1 and 2. Two of these states – Nebraska and Kansas – exceeded the AAP recommendations by requiring five visits.
- Forty-eight states met AAP recommendations for three well-child visits for a child between the ages of 3 and 5. Three states – Arkansas, California and Delaware – require only two visits for these children.
The federal government set a benchmark for 80 percent of Medicaid-enrolled children to receive at least one developmentally-appropriate health screen each year during a well-child visit. In 2008:
- 40 states reported that they completed the screens of more than 80 percent of children less than 1 year old;
- 44 states reported that they completed the screens of more than 80 percent of children ages 1 to 2 years; and
- 20 states reported that they completed the screens of more than 80 percent of children ages 3 to 5.
Newborn Screening
Universal newborn screening for hearing and metabolic deficiencies and disorders are recommended for all children in order to identify and treat conditions that can cause life-long disabilities. The March of Dimes and American Academy of Pediatrics recommend newborn screens for hearing and 28 metabolic conditions. Currently, some states are still failing to perform all of these recommended screens.
- Forty-one states require universal newborn screening for the 28 metabolic deficiencies/disorders as defined by the March of Dimes; an increase of 21 states since 2007.
- Thirty-six states require universal newborn screening for hearing deficiencies, with two additional states – Michigan and South Carolina – requiring the screening since 2007.
Part C Early Intervention Services
Children who exhibit or show risk of developmental delays in the first three years of life are at higher risk of school failure, mental health problems, and other conditions that limit their life opportunities. Part C of the Individuals with Disabilities Education Act (IDEA) requires states to provide early intervention services to children from birth to age 3 who have an identified disability or serious delay. Some states also extend eligibility to infants and toddlers who are at risk of a serious delay due to individual or family risk factors, such as low birth weight, parent mental illness and high exposure to lead in the home. These risk factors are more commonly experienced by low-income children than their more advantaged peers. Recent research suggests that both a child’s poverty status and a state’s use of narrow eligibility criteria increase the chance that a child with a parent-reported delay or disability will not receive early intervention.
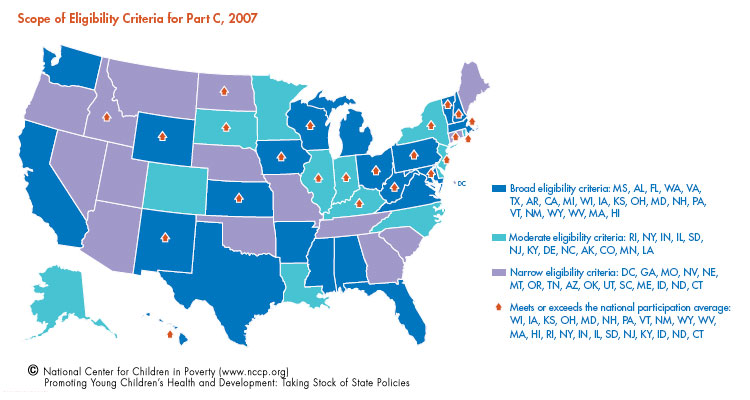
The Department of Education classifies states as using narrow, moderate or broad eligibility criteria for early intervention (EI) services. In general, states with broad and moderate criteria extend eligibility to include children who have less serious delays or who show risk factors for delays or disabilities. Nationally, an average of 2.5 percent of children birth through age 2 receives Part C early intervention services. States with broad and moderate eligibility criteria are more likely to be above the national average in the numbers of children who receive EI services compared to states with a narrow definition. Data released in 2008 (the most current available) show that:
- twenty-two states use a broad definition of eligibility that includes children “at-risk” of serious delays and disabilities, 13 states use a moderate definition, and 16 states have narrow definitions; and
- among states with a broad definition, 59 percent (13 states) serve more children than the national average; among states with moderate definitions, 54 percent (seven states) serve more children than the national average; and among states using a narrow definition, 19 percent (three states) serve more than the national average.
States’ Part C early intervention programs are increasingly focused on identifying the mental health needs of very young children. However, efforts to identify mental health needs appear stronger in the screening process than in evaluations to determine eligibility for EI services.
- More than half (58 percent) of the 48 states whose Part C coordinators responded to a recent survey reported that their state recommended the use of an instrument that screens for social-emotional problems.
- More than half of the responding states (56 percent) also reported that they do not require the participation of a professional with expertise in young children’s social-emotional development in the multi-disciplinary evaluation that is conducted to determine eligibility for EI services.
What States Can Do
Full implementation of national health care reform under the Patient Protection and Affordable Care Act (PPACA) will occur in stages over the next several years. Some provisions, such as federal subsidies for families to help them buy health insurance, and the creation of health insurance exchanges designed to provide affordable options to families who do not qualify for public insurance, will not be fully in place until 2014. Meanwhile, states should consider the following steps to ensure that low-income young children receive the health care they need for positive health, developmental, and educational outcomes.
- PPACA requires that states maintain their Medicaid and CHIP programs through at least 2019. While states cannot lower income eligibility thresholds during this period, they can and should extend coverage to young children in families with incomes below 200 percent of the federal poverty line, regardless of immigration status. Coverage for undocumented children will require the use of separate state funds even after full implementation of PPACA.
- By 2014, the PPACA will require that states provide Medicaid coverage to all adults with incomes up to 133 percent of FPL. Low-income pregnant women with income between 133 percent and 200 percent of FPL will still be left without coverage under PPACA, along with low-income, pregnant, undocumented immigrant women. To ensure rising rates of healthy births and infants who start life without disabilities, states should extend Medicaid coverage to all pregnant women, regardless of immigration status, with incomes up to 200 percent of FPL. Separate state funding should be used for coverage of undocumented immigrant women.
- States should consider several actions to ensure that pregnant women and children have the timely and continuous care they need for positive child health and developmental outcomes: (1) provide 12-month continuous eligibility for both Medicaid and CHIP for children; (2) provide presumptive eligibility for public insurance coverage for both children and pregnant women; and (3) keep co-pays low so that families are not deterred from seeking care.
- State policy initiatives designed to strengthen supports for young children’s healthy development and school readiness should establish new guidelines, training for pediatric settings and monitoring procedures to ensure that all recommended well-child visits and developmental screenings are provided for children birth to age 5. The Early Childhood Comprehensive Systems initiatives funded by the federal Maternal and Child Health Bureau and the State Early Childhood Advisory Councils, required under the Improving Head Start for School Readiness Act of 2007, provide opportunities for developing these supports for young children’s well-being.
- States that currently do not conduct the recommended universal newborn screens for 28 metabolic deficiencies/disorders and hearing problems should join the majority of states that currently require these screens.
- States that use narrow eligibility criteria in their Part C Early Intervention Programs should consider broadening their eligibility criteria to include children at-risk of serious delays and disabilities. Early interventions with at-risk children can reduce the chance of costly long-term conditions that limit children’s prospects for good health and educational outcomes.
- States’ Part C programs should strengthen their capacity to respond to young children’s mental health needs by requiring the participation of a professional with expertise in infant-toddler social-emotional development during the multidisciplinary evaluation that determines eligibility for EI services.
*Birth to age 5 is inclusive through the fifth year.
1. Fomby, Paula; Cherlin, Andrew J. 2007. Family Instability and Child Well-being. American Sociological Review 72(2): 181-204(24).
Rouse, Heather; Fantuzzo, John W. 2009. Multiple Risks and Educational Well Being: A Population-Based Investigation of Threats to Early School Success. Early Childhood Research Quarterly 24(1): 1-14.
Thompson, Ross; Raikes, H. Abigail. From Knitzer, Jane; Kauffman, R.; Perry, D. (eds). Early Childhood Mental Health. Baltimore, MD: Paul H. Brookes Publishing Co.
2. Currie, Janet. 2005. Health Disparities and Gaps in School Readiness. The Future of Children 15(1): 117-138.
3. McLaughlin, Andrea E.; Campbell, Frances A.; Pungello, Elizabeth P.; Skinner, Martie. 2007. Depressive Symptoms in Young Adults: The Influences of the Early Home Environment and Early Educational Child Care. Child Development 78(3): 746-756.
4. Sanchez, Katherine; Gomez, Rebecca; King, Davis. 2010. Fostering Connections and Medical Homes: Addressing Health Disparities Among Children in Substitute Care. Children and Youth Services Review 32(2): 286-291.
Silver, Ellen Johnson; Heneghan, Amy M.; Bauman, Laurie J.; Stein, Ruth E. 2006. The Relationship of Depressive Symptoms to Parenting Competence and Social Support in Inner-city Mothers of Young Children. Journal of Maternal and Child Health 10(1): 105-112.
5. Ross, Donna Cohen; Marks, Caryn. 2009. A Foundation for Health Reform: Findings of a 50 State Survey of Eligibility Rules, Enrollment and Renewal Procedures, and Cost-Sharing Practices in Medicaid and CHIP during 2009. Kaiser Commission on Medicaid and the Uninsured, The Henry J. Kaiser Family Foundation. www.kff.org (accessed Feb. 28, 2010).
6. Sacks, Kevin. 2010. Arizona Drops Children’s Health Program. The New York Times. www.nytimes.com/2010/03/19/health/policy/19arizona.html(accessed: April 1, 2010).
8. Hamilton, Erin; Hummer, Robert; You, Xiuhong; Padilla, Yolanda. 2006. Health Insurance and Health-care Utilization of U.S.-Born Mexican-American Children. Social Science Quarterly 87(5): 1280-1294.
Padilla, Yolanda; Hamilton, Erin; Hummer, Robert. 2009. Beyond the Epidemiological Paradox: The Health of Mexican- American Children at Age Five. Social Science Quarterly 90(5): 1072-1088.
Zhihuan, Jennifer Huang; Yu, Stella M.; Ledsky, Rebecca. 2006. Health Status and Health Service Access and Use Among Children in U.S. Immigrant Families. American Journal of Public Health April 96(4): 1-8.
9. Reardon-Anderson, Jane; Capps, Randy; Fix, Michael. The Health and Well-Being of Children in Immigrant Families. 2002. New Federalism, The Urban Institute, Series B, No. B-52.
10. The Henry J. Kaiser Family Foundation. 2009. New Option for States to Provide Federally Funded Medicaid and CHIP Coverage to Additional Immigrant Children and Pregnant Women. Kaiser Commission on Key Facts. www.kff.org (accessed Nov. 11, 2009).
12. Szilagyi, Peter G.; Cheng, Tina; Simpson, Lisa; Berkelhamer, Jay E.; Sectish, Theodore C. 2008. Health Insurance for All Children and Youth in the United States: A Position Statement of the Federation of Pediatric Organizations. The Journal of Pediatrics 153(3): 301-302.
13. Allred, Norma J.; Wooten, Karen G.; Kong, Yuan. 2007. The Association of Health Insurance and Continuous Primary Care in the Medical Home on Vaccination Coverage for 19- to 35-Month-Old Children. Pediatrics 119: S4-S11.
American Academy of Pediatrics, Committee on Child Health Financing. 2002. Policy Statement: Organizational Principles to Guide and Define the Child Health Care System and/or Improve the Health of All Children. Pediatrics110(1): 132-135.
Levine, Phillip B.; Schanzenbach, Diane. 2009. The Impact of Children’s Public Health Insurance Expansions on Educational Outcomes. Forum for Health Economics & Policy 12(1).
Perry, Cynthia D.; Kenney, Genevieve M. 2007. Preventive Care for Children in Low-income Families: How Well Do Medicaid and States’ Children Health Insurance Programs Do? Pediatrics 120(6):1393-1401.
14. Kenney, Genevieve. 2007. The Impacts of the State Children’s Health Insurance Program on Children Who Enroll: Findings from Ten States. Health Services Research 42(4): 1520–1543.
15. NCCP Calculations of Child and Adolescent Health Measurement Initiative (CAHMI). 2007 National Survey of Children’s Health Indicator Dataset. Data Resource Center for Child and Adolescent Health.
23. Marrow, Beth. Express Lane Activities: States On The Move. February 2010. The Children’s Partnership. http://www.childrenspartnership.org/AM/Template.cfm?Section=State_Activity_Report&TEMPLATE=/CM/ContentDisplay.cfm&CONTENTID=13347(accessed April 2010)
24. Sibai, Baha; Dekker, Gus; Kupferminc, Michael. 2005. Preeclampsia. The Lancet 365(9461, 26): 785-799.
25. Roberts, G.; Bellinger, D.; McCormick, M. C. 2007. A Cumulative Risk Factor Model for Early Identification of Academic Difficulties in Premature and Low Birth Weight Infants. Maternal and Child Health Journal 11(2): 161-72.
Stein, Ruth E. K.; Siegel, Michele J.; Bauman, Laurie J. 2006. Are Children of Moderately Low Birth Weight at Increased Risk for Poor Health? A New Look at an Old Question. Pediatrics (1): 217-223.
33. Recommendations for Preventive Pediatric Healthcare. 2008. American Academy of Pediatrics http://pediatrics.aappublications.org/cgi/data/120/6/1376/DC1/1 (accessed March 29, 2010).
34. U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services. 2009. The Annual EPSDT Report (Form CMS-416). www.cms.hhs.gov/MedicaidEarlyPeriodicScrn/03_StateAgencyResponsibilities.asp(accessed Nov. 18, 2009)
37. Health Care Financing Administration (HCFA), July 1990. http://oig.hhs.gov/oei/reports/oei-07-90-00130.pdf (accessed March 29, 2010).
40. National Newborn Screening and Genetics Resource Center. 2009. National Newborn Screening Status Report. http://genes-r-us.uthscsa.edu(accessed Oct. 23, 2009).
44. McLeod, Jane D.; Fettes, Danielle L. 2007. Trajectories of Failure: The Educational Careers of Children with Mental Health Problems. The American Journal of Sociology 113(3): 653-701.
Wolke, Dieter; Schmid, Gabriele; Schreier, Andrea; Meyer, Renate. 2009. Crying and Feeding Problems in Infancy and Cognitive Outcome in Preschool Children Born at Risk: A Prospective Population Study. Journal of Developmental & Behavioral Pediatrics 30(3):226-238.
Feldman, Maurice A.; Hancock, Christie L.; Rielly, Nicole; Minnes, Patricia; Cairns, Colleen. 2000. Behavior Problems in Young Children With or At Risk for Developmental Delay. Journal of Child and Family Studies 9(2):247-261.
45. McManus, Beth; McCormick, Marie C.; Acevedo-Garcia, Dolores; Ganz, Michael; Hauser-Cram, Penny. 2009. The Effect of State Early Intervention Eligibility Policy on Participation Among a Cohort of Young CSHCN. Pediatrics124(4): 368-374.
46. U.S. Department of Education, Office of Special Education Programs, Data Analysis System (DANS). 2008. Infants and Toddlers Receiving Early Intervention Services in Accordance with Part C.
48. Cooper, Janice; Vick, Jessica. 2009. Promoting Social-emotional Well-being in Early Intervention Services. New York, NY: National Center for Children in Poverty, Columbia University Mailman School of Public Health.
50. Schwartz, Karen. Kaiser Commission on Medicaid and the Uninsured: COBRA Subsidy for the Uninsured. April 2010. The Henry J. Kaiser Family Foundation. http://www.kff.org/uninsured/upload/7875-02.pdf (accessed April 20, 2010)
51. Summary of Medicaid, CHIP, and Low-Income Provisions in Health Care Reform. April 2010. Center for Children and Families, Georgetown University Health Policy Institute.
52. Focus on Health Reform: Health Reform Implementation Timeline. March 31, 2010. The Henry J. Kaiser Family Foundation.